In collaboration with Jordi Tarascó Palomares, General Surgeon and Digestive System Specialist. Specialist in Endocrine, Bariatric, and Metabolic Surgery.
Robotic surgery represents the forefront of modern surgical techniques, offering patients safer and minimally invasive procedures. However, the current training process for robotic surgery is slow and comes with certain limitations, leaving a gap in meeting the high demand for trained professionals.
Da Vinci Surgical Platform
The Intuitive da Vinci robotic platform is one of the most established and powerful revolutions in the field of minimally invasive surgery, offering surgeons greater precision, comfort, ergonomics, and safety, resulting in better outcomes for patients. This platform features a vision tower with a 2D monitor, the patient cart with robotic arms, and the surgeon’s console, which may include a second console for educational and proctoring purposes. The particularity of this system is that the surgeon’s vision through the console is an immersive 3D view of the intervention. Meanwhile, the assistant surgeon, responsible for changing the surgical instruments on the robot’s arms, must follow the intervention from the 2D monitor in the vision tower.

Current Training Programs in Robotic Surgery
Currently, training in robotic surgery is quite standardized and can be divided into four phases. It begins with an initial phase where theoretical knowledge must be acquired and certified through examinations. In the second phase, simulation hours are conducted on the console, based on games and small challenges to improve hand-eye coordination through the robot’s console. Thirdly, the concept of case observation emerges, where trainees attend interventions performed by expert surgeons, both nationally and internationally, to witness step by step the execution of a robotic intervention, the challenges they will face, and how to overcome them. In the fourth phase, the trainee surgeon who is going to perform their first robotic surgery case is accompanied or tutored (proctored) by more experienced surgeons until they gain the necessary experience to perform it autonomously and safely.
Limitations of Current Training
Despite the significant advances made in the field of minimally invasive robotic surgery, there are still some key aspects to improve, especially in terms of training:
- In the case observation phase, only the primary surgeon performing the intervention has immersive vision. The rest of the colleagues and trainees must look through the 2D monitor or accessory screens, resulting in a loss of information.
- Logistics problems arise from the travel of trainee surgeons from their home hospital to the location of the intervention. These travels can be both national and international, increasing the cost in terms of time and resources for hospitals.
- Due to the imperative need to maintain aseptic conditions, there is a limited capacity within operating rooms, thus limiting the number of attendees who can witness the intervention.
- Moreover, when it is the tutor who travels to train the trainees, the hospital in many cases lacks the second da Vinci console, designed for tutoring cases, resulting in guidance and instruction being received through a 2D monitor, generating a suboptimal training experience.
With all these issues, the training process has become tremendously slow and does not meet the high demand for training currently existing in the field of robotic surgery.
mSurgery Collaborative Platform
Due to the limitations, the implementation of complementary technological tools becomes necessary to contribute to the training of these cutting-edge techniques. In this way, the mSurgery platform becomes a facilitating tool for robotic surgery training by having:
- Dynamic grid that allows simultaneous visualization of multiple video sources with resolutions up to 4K.
- 3D vision of the operating area.
- Support for new virtual reality, mixed reality technologies, as well as 360º cameras.
- Generation of a repository of recorded sessions for continuous review.
- Accessibility: Multi-device platform.

The combination of all its features results in the following functionalities and advantages:
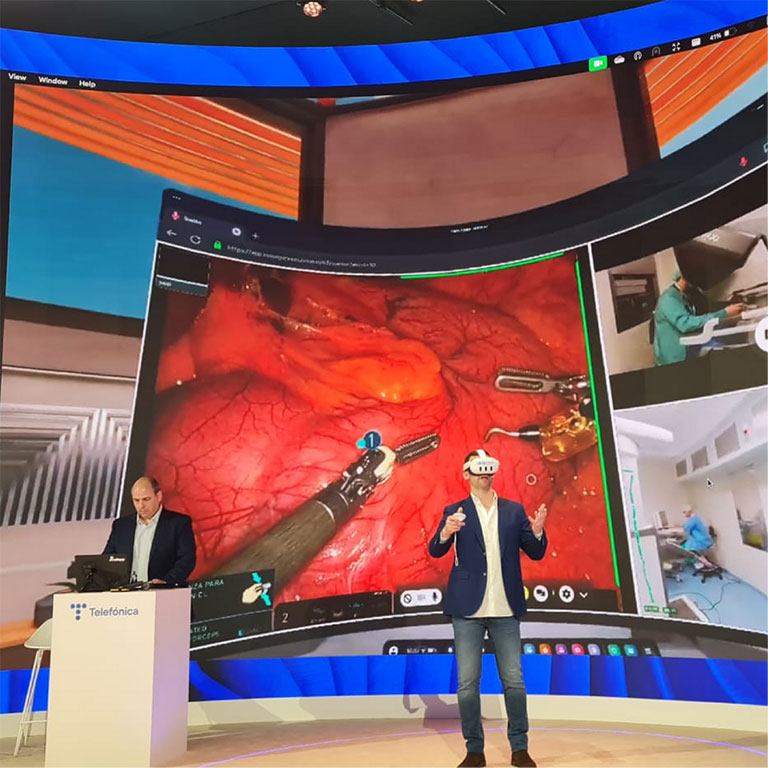
Telepresence: The platform enables the combination of virtual reality glasses with the integration of 360 cameras, offering the sensation of being inside the operating room itself. This allows for visual and verbal interaction with all components of the operating room, providing a complete context of what is happening in the intervention.
Stereoscopy: The platform offers the possibility of experiencing the same 3D or stereoscopic vision as the primary surgeon’s console, through any device that allows its visualization, such as virtual reality glasses. Likewise, a da Vinci console can be virtually generated, allowing you to get the feeling of approaching the console viewer and experiencing the same immersive vision as the surgeon.
Distance and Bidirectionality: It allows for remote attendance at interventions with a sensation similar to being present in the operating room without the need for national and international travel, offering bidirectional communication between student and tutor.
Massive and Real-time: Live broadcast of surgical sessions to a large number of surgeons or attendees simultaneously in real-time, eliminating spatial limitations.
Conclusion
In this way, an extremely powerful training tool in robotic surgery is obtained, which contributes to meeting the current high demand for training, generating a high-quality training program that is more accessible and allows for faster and more homogeneous distribution of surgical techniques.